Invisible Agony of Sickle Cell Disease (SCD)
Our veteran writer on Community Health Affairs *Dr Naresh Purohit, (Executive Member of the Thalassaemia and Sickle Cell Society (TSCS) delves into the causes, demographic prevelance and preventive actions desired against this common and ignored disease!
New Delhi/Bhopal : Sickle-cell disease is an autosomal recessive inherited haemoglobin disorder. It is the r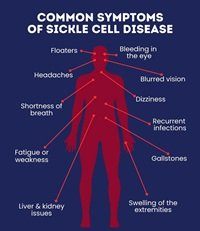 esult of a genetic mutation occurring in communities that originally inhabited areas affected by endemic malaria. Over time, the gene corresponding to haemoglobin in their bodies mutated to resist plasmodium, the parasite that causes malaria. This changed the shape of red-blood cells from round to sickle-shaped. As a result, these people experience pain, eye problems, infections, even stroke and potential damage to multiple organs in the body.
esult of a genetic mutation occurring in communities that originally inhabited areas affected by endemic malaria. Over time, the gene corresponding to haemoglobin in their bodies mutated to resist plasmodium, the parasite that causes malaria. This changed the shape of red-blood cells from round to sickle-shaped. As a result, these people experience pain, eye problems, infections, even stroke and potential damage to multiple organs in the body.
Different forms of the same gene are called alleles. If a person has two alleles of the defective haemoglobin gene, they’re said to have homozygous sickle-cell disease. If they have only one defective allele, they’re said to have heterozygous sickle-cell disease.
People with the homozygous variety experience the typical symptoms of sickle-cell anaemia and have lower life-expectancy. Those with heterozygous sickle-cell anaemia live relatively healthy lives – but can pass on the gene to their offsp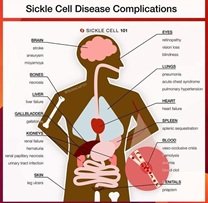 ring.
ring.
In India, sickle-cell anaemia is largely found among tribal, Dalit and a few OBC communities, and to a lesser extent among people of other communities.
It’s a neglected disease that affects a neglected people. Sickle cell disease is highly prevalent in certain parts of India, especially the Central Deccan region, which is popularly known as the “Sickle Belt”. One fifth of the population in Madhya Pradesh consists of tribal population. It is estimated that the prevalence of sickle cell gene within the tribal community ranges from 10% to 33%.
Over 1 crore people have been screened under the National Sickle Cell Anemia Elimination Mission (2023). There is no consolidated government data on the disease’s exact prevalence; instead, there have been sporadic efforts by individual medical researchers and institutions. One scientific study estimated that the disease’s prevalence in India’s states ranges from 0% to 40%. The prevalence also varies between communities, which means there needs to be community-focused strategies for data collection and intervention.
In India, 20% of children with the disease die before they turn 5 and 30% don’t reach adultho od. One NGO Jan Swasthya Sahyog of Madhya Pradesh from 2018- 2021 reported that 60% of those with sickle-cell disease are school-goers, and only 0.8% of those with the disease were older than 50 years.
od. One NGO Jan Swasthya Sahyog of Madhya Pradesh from 2018- 2021 reported that 60% of those with sickle-cell disease are school-goers, and only 0.8% of those with the disease were older than 50 years.
Agonising pain is the most intractable problem encountered by patients with sickle cell disease (SCD). It is unpredictable, persistent, severe and recurrent. Patients with SCD encounter acute, chronic and neuropathic pain. Of these, the acute pain of vaso-occlusive crisis is the most debilitating and is also the commonest cause of hospitalization among children and adults with SCD. Adults living with SCD report pain on 55% of the days annually and around 29% patients report daily pain . In pediatric patients, pain is responsible for 50-60% of the emergency room visits and 60-80% of hospitalizations . Pain interferes with the ability to participate in activities of daily living, causing 44% to drop out of a school program with an average of 7 times greater absence from school than a regular child .
The agony of sickle cell disease unfortunately is “invisible”; many patients are under diagnosed and undertreated. Many are labelled as “drug seekers” as opioid addiction as well as underdosing due to the fear of dependence is a reality. It is also difficult to objectify pain, and subjective reporting with unidimensional tools such as numerical scales or faces pain scale are often used .
Sickle cell pain can be managed by pediatricians and physicians in primary care settings effectively. In children presenting with pain, management should be initiated quickly along with hydration, oxygen, muscle relaxants (if  needed) and other non- pharmacological approaches. They should be thoroughly assessed for associated medical issues such as infection, acute chest syndrome, trauma and splenic sequestration which often trigger the pain . There is no one-size-fits-all strategy for managing pain in SCD. Pain is managed mostly based on the WHO pain ladder , which progresses from non-pharmacological adjuvant therapies to non-opioids to weak opioids to strong opioids for severe pain. Weak oral opioids such as tramadol and codeine are not recommended for use in children.
needed) and other non- pharmacological approaches. They should be thoroughly assessed for associated medical issues such as infection, acute chest syndrome, trauma and splenic sequestration which often trigger the pain . There is no one-size-fits-all strategy for managing pain in SCD. Pain is managed mostly based on the WHO pain ladder , which progresses from non-pharmacological adjuvant therapies to non-opioids to weak opioids to strong opioids for severe pain. Weak oral opioids such as tramadol and codeine are not recommended for use in children.
It is to be noted that most patients reaching the emergency department would have already tried pain relief at home. Hence, a quick triaging followed by initiation of appropriate pain relief is crucial. Morphine is the most commonly used intravenous (IV) opioid in this setting. Use of morphine needs appropriate training of nurses and doctors in the team, with continuous cardiorespiratory monitoring . Often it also requires patient controlled delivery in addition to a basal continuous IV infusion to improve the time to pain relief, thus resulting in better satisfaction and earlier discharge.
As per the 2020 American Society of Hematology (ASH) recommendations for the management of pain in SCD in children and adults, a short course of 5-7 days of non-steroidal anti-inflammatory drugs (NSAIDs) in addition to opioids is advised . It is in this context that the use of non-opioids has been tested, especially in low-resource countries to explore options to deliver similar pain relief with less intensive supportive care. Non-opioids include IV acetaminophen or ketorolac, or oral ibuprofen, naproxen or meloxicam.
They are also often helpful to transition from IV opioids to oral medicines in order to plan co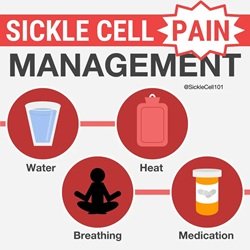 ntinuation of care at home. Ketorolac has been tested earlier against opioids in SCD with variable results .
ntinuation of care at home. Ketorolac has been tested earlier against opioids in SCD with variable results .
Pain in chronic hematological diseases has serious life challenges. : In the setting of limited morphine availability and accessibility in India, pain relief with ketorolac should improve access to care for the vast majority suffering in the community. The recognition of pain, as well as the delivery of pain relief has been a challenge and medical practices aimed at shortening time to action are welcome in this context. As more children with SCD survive into adulthood, the need for improving acute care delivery becomes crucial.
*Dr. Naresh Purohit-MD, DNB, DIH, MHA, MRCP(UK), is an Epidemiologist,  and Advisor-National Communicable Disease Control Program of Govt. of India, Madhya Pradesh and several state Health organizations. He’s the Principle Investigator – Association of Studies In Behavioural Science), Dr. Purohit is also Advisor-National Mental Health Program .
and Advisor-National Communicable Disease Control Program of Govt. of India, Madhya Pradesh and several state Health organizations. He’s the Principle Investigator – Association of Studies In Behavioural Science), Dr. Purohit is also Advisor-National Mental Health Program .
