Sickle Cell Disease Needs Urgent Attention
World Sickle Cell Awareness Day - 19 June
Our Community Health expert, *Dr Naresh Purohit, (Executive Member- Indian Association of Palliative Care), draws attention to mutation in RBC prevalent in Sickle Belt of India !
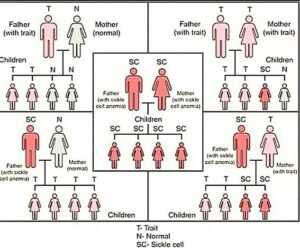
New Delhi/Bhopal: Sickle cell disease is one of the commonest hemoglobinopathy worldwide. It is, an  autosomal recessive inherited haemoglobin disorder, in which there is the replacement of valine in place of glutamine on the beta globin chain, causing a structural modification in the shape of RBCs and thus leading to the sickle like shape of Red Blood Cells (RBCs). These sickle red cells are prone for haemolysis and are “sticky”. The sticking together of sickle RBCs, or “sickling” leads to microvascular thrombosis, inflammation, haemolysis and vascular blockage.
autosomal recessive inherited haemoglobin disorder, in which there is the replacement of valine in place of glutamine on the beta globin chain, causing a structural modification in the shape of RBCs and thus leading to the sickle like shape of Red Blood Cells (RBCs). These sickle red cells are prone for haemolysis and are “sticky”. The sticking together of sickle RBCs, or “sickling” leads to microvascular thrombosis, inflammation, haemolysis and vascular blockage.
Sickle cell. disease is highly prevalent in certain parts of India, especially the Central Deccan region, which is popularly known as the “Sickle Belt”. One fifth of the population in Madhya Pradesh consists of tribal  population. It is estimated that the prevalence of sickle cell gene within the tribal community, ranges from 10% to 33 %.
population. It is estimated that the prevalence of sickle cell gene within the tribal community, ranges from 10% to 33 %.
Most often, the patients from these tribal populations are uneducated, poor, and reside in interior areas which make it difficult for them to access healthcare as they do not have the capacity to afford frequent doctor visits or access even simple drugs like hydroxyurea etc. All of these factors lead to delayed diagnosis, poor drug compliance and ultimately to patients landing up with, complications of sickle cell disease.
Patients with sickle cell disease live with significant morbidity due to pain which. adversely affects their quality of life. This pain can present as either acute, acute on chronic or persist as chronic pain. The incidence and severity of pain usually increases with age as complications of the disease advances. These episodes of pain can occur due to various reasons such as inflammation,. tissue hypoxia and reperfusion injury, ischemia due to capillary occlusion and many other neuropathic pain mechanisms like central sensitization.
Pain control in these patients usually requires individualized, multi-modality approaches including pharmacological, Non- pharmacological and Interventional pain treatments. In acute pain, it is recommended to have a rapid and frequent assessment of pain and titrate the analgesics accordingly. Analgesics are advised 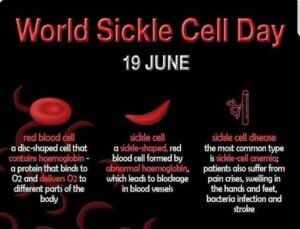 as per the WHO Analgesic ladder. NSAIDS like Ibuprofen and Ketorolac are preferred first line analgesic agents. However, these drugs should be. avoided for long term with fear of end organ toxicities. Corticosteroids may reduce opioid requirement in acute pain, but generally not recommended in sickle cell disease related acute pain as cessation has been associated with rebound pain and other complications.
as per the WHO Analgesic ladder. NSAIDS like Ibuprofen and Ketorolac are preferred first line analgesic agents. However, these drugs should be. avoided for long term with fear of end organ toxicities. Corticosteroids may reduce opioid requirement in acute pain, but generally not recommended in sickle cell disease related acute pain as cessation has been associated with rebound pain and other complications.
Hydroxyurea has proven to be useful in preventing recurring episodes of pain. IV hydration, chronic transfusions and erythrocytopheresis are to be considered based on the opinion of the haematologist.
Opioid medications can. be used in acute pain either as intermittent or continuous infusions based on the frequency of pain. The pain controlled analgesia option can be preferred in acute and varying pain conditions. Chronic use of opioids is usually discouraged unless pain is refractory to other modes of treatment. In these patients, opioids are required for long term, however, it should be prescribed in the lowest effective dose with frequent behavioural risk assessments. In patients with opioid resistant pain, subanaesthetic. infusion of ketamine in dosage of 0.1mg/kg/hr upto 1 mg/kg/hr can be considered. Regional anaesthesia like epidural or peripheral nerve blocks can be considered based on anatomical location of pain in frequent acute or persistent pain conditions.
 Although pain is an overtly visible symptom in these patients’, the chronicity of this illness affects various domains of overall health and growth of young people. Dropping out from education, delayed growth and bony abnormalities. affect the social wellbeing of such patients’. Recurrent, severe infections and ischaemic events may lead to sudden unexpected death.
Although pain is an overtly visible symptom in these patients’, the chronicity of this illness affects various domains of overall health and growth of young people. Dropping out from education, delayed growth and bony abnormalities. affect the social wellbeing of such patients’. Recurrent, severe infections and ischaemic events may lead to sudden unexpected death.
*Dr. Naresh Purohit-MD, DNB, DIH, MHA, MRCP(UK), is an Epidemiologist,  and Advisor-National Communicable Disease Control Program of Govt. of India, Madhya Pradesh and several state Health organizations. Dr. Purohit is also Chief Advisor Hospitals Association of India and Chief Investigator Association of Studies for Kidneycare.
and Advisor-National Communicable Disease Control Program of Govt. of India, Madhya Pradesh and several state Health organizations. Dr. Purohit is also Chief Advisor Hospitals Association of India and Chief Investigator Association of Studies for Kidneycare.

Comments are closed.